
"Quit Smoking" also ranks very high in the New Year's resolution statistics. If you are still looking for an excuse to not stop smoking “the smoking
paradox” could be it!
[1] Kufner et al, Stroke, 2013
[2] Grines et al, Circulation, 1995
[3] Aune et al, BMC Med, 2011
[4] Newby et al, Circulation, 2011
[5] Barua et al, Arterioscler Thromb Vasc Biol, 2010
by Anna Kufner, PhD Student AG Ebinger
This article was originally published June 2015 in Volume 08, Issue 02 " Art. And the Brain."
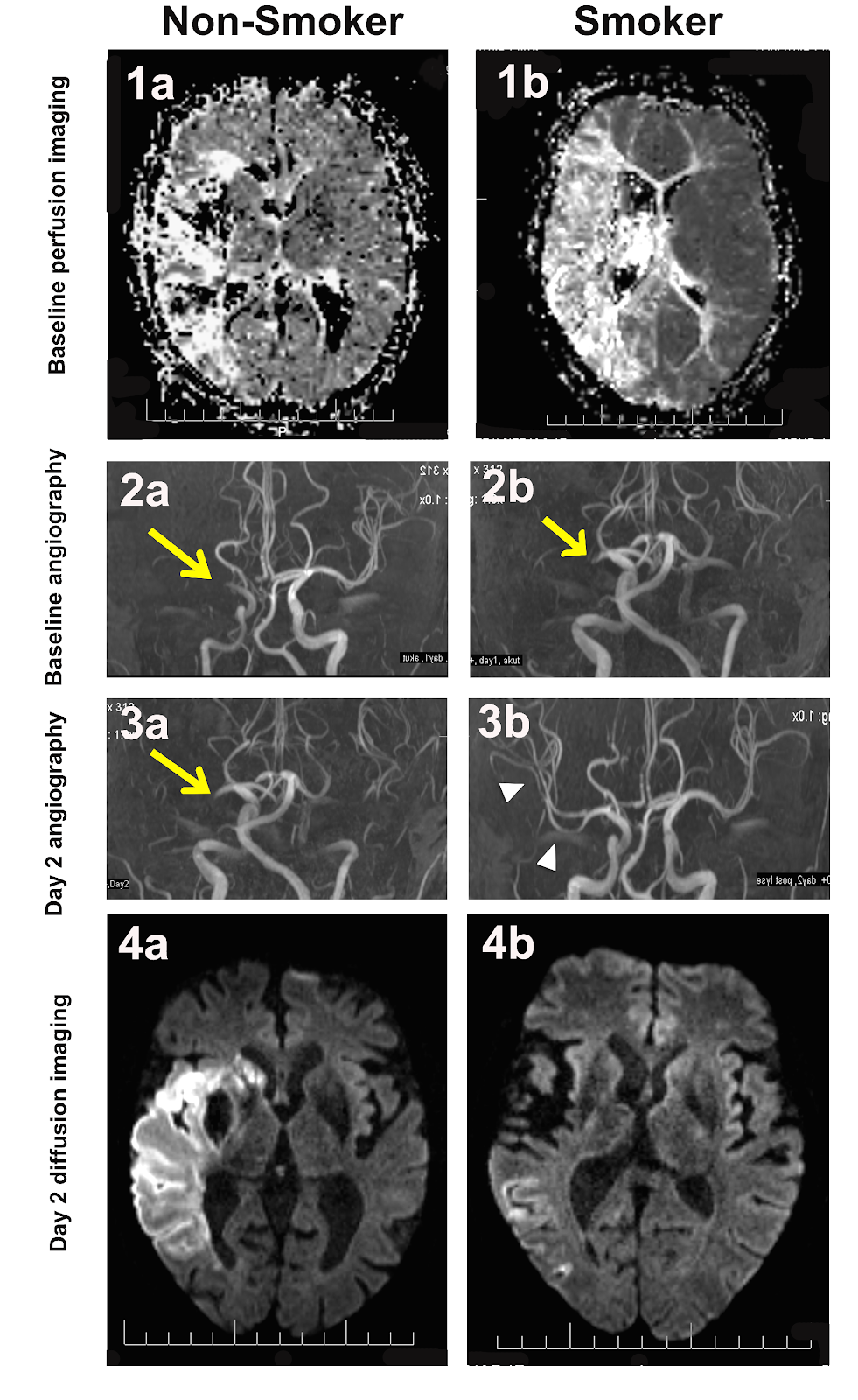 |
Acute and post-treatment day2 images of a non-smoker
(left) and smoker
(right) following middle cerebral artery
occlusion. Acute perfusion
images of non-smoker (1a)
and smoker (1b) are similar. Angiographies of
both patients
show identical vessel occlusion (arrow, 2a 2b). Following
thrombolysis, non-smoker still has occluded vessel (3a),
yet smoker has
recanalized (3b) showing distal blood flow
restored (arrow heads).
Follow-up diffusion image of
non-smoker shows larger lesion (4a)
compared to
non-smoker (4b).
|
A
recent study conducted at the Charité re-awakened a hot topic of
controversy first described nearly 20 years ago, termed “the smoking
paradox” in which smokers respond better to treatment following ischemic
cardiovascular events [1].
Smoking
is a well-known risk factor for atherosclerosis, myocardial infarction
(MI; heart attack) and ischemic stroke. Therefore, it is understandable
why the community was unsettled by results published in an observational
study in 1995 describing lower mortality rates in smokers with MI
following treatment [2].
MI
and ischemic stroke are caused by an obstruction of a blood vessel due
to a thrombus, or blot clot. The diminished blood flow distal to the
occluded vessel causes the downstream tissue to die due to ischemia. The
main treatment of these ischemic events is either mechanical removal of
the blot clot or lysis of the clot via systemic thrombolysis.
Following
the first study reporting the smoking-paradox in 1995, several studies
followed showing similar results. However, a critical review of these
studies put a quick end to the discussion; this review attributed the
observed better outcome in smokers to their younger age and to
insufficient statistical power [3]. Subsequently, the once-hot topic of
the smoking paradox fell silent for several years until a recent Charité
study stirred up the discussion again with robust results.
In
the neuroimaging study at the Charité, smokers with ischemic stroke
showed a 6-fold greater chance of recanalization (opening of the
occluded artery in response to thrombolysis; see figure) and a trend
towards a better recovery compared to non-smokers [1].
STROKE
TREATMENT MORE
EFFECTIVE IN SMOKERS
Before
the study was even accepted for publication, researchers at the Charité
got wind of the results and began questioning the findings. Not until
an external statistician reviewed the data did the study get
the permission to proceed to be re-submitted.
Once accepted for publication in Stroke,
the critiques began with similar arguments against the studies in the
90s, namely that statistical power was lacking. It is difficult to argue
against these criticisms with one retrospective study. However, it
wasn’t long before four further studies followed supporting the theory: smokers respond better to treatment than non-smokers. Although these findings may appear paradoxical at first, there is a feasible scientific explanation.
Experimental
animal studies show that smoking decreases the amount of endogenous
tissue-plasminogen-activator (tPA) released from endothelial cells [4];
tPA is a protein involved in the breakdown of fibrin, which causes blood
to clot. Higher fibrin levels in smokers compared to non-smokers [5]
may cause higher risk for thrombus formation. Therefore, the clots
formed in smokers may have a higher fibrin content compared to
non-smokers, making them more susceptible to be lysed by exogenous tPA
treatment (i.e. thrombolysis).
In
light of this possible explanation, the term “smoking paradox” rings
quite true. On the one hand, smokers have a higher chance of having a
stroke in the first place, but on the other hand have a greater chance
of responding to treatment. So, how does this help us in the clinical
setting?
PARADOX LINKED TO
CLOTS'
HIGHER FIBRIN CONTENT
Thrombolysis
with tPA is not risk-free: approximately 6% of patients suffer an
intracerebral hemorrhage. Furthermore, only a small percentage of
patients with ischemic stroke arrive to the clinic within the
therapeutic time-window of 4.5 hours. Nonetheless, off-label treatment
with tPA in tricky cases is quite common. If we know smokers are more
likely to respond to treatment, we might have an indication for
thrombolysis in potentially difficult cases (i.e. elderly patients,
patients arriving in later time-windows).
As
of yet, there are only small studies on this topic and results remain
controversial. However, recently two large multicenter studies have been
launched in order to further investigate the smoking paradox
phenomenon, each including >6,000 patients. Hopefully, these studies
will unveil the true “smoking effect” and answer the dozens of
unanswered questions regarding how we can apply this knowledge in the
clinical setting.
[2] Grines et al, Circulation, 1995
[3] Aune et al, BMC Med, 2011
[4] Newby et al, Circulation, 2011
[5] Barua et al, Arterioscler Thromb Vasc Biol, 2010
by Anna Kufner, PhD Student AG Ebinger
This article was originally published June 2015 in Volume 08, Issue 02 " Art. And the Brain."
No comments:
Post a Comment